On flattening the curve
C19.Life • 20 October 2024
❦ If parents, and politicians and teachers, and healthcare workers and public health bodies wanted things to change, all they need do is read.
It’s all there.
But they don’t. They won’t.
And they insist on their medical and scientific flat-earthing – hand-sanitiser for aerosol-transmitted disease – because they prefer the world to be flat.
So let them walk off the edge of the world.
[Caveat: The earth is not flat, and doing nothing will not flatten the curve – but walk far enough, and you are likely to fall off a cliff.]
© 2024
C19.Life
✾
Read... or walk...
The Health and Safety Executive (HSE) has designated SARS-CoV-2, the virus that causes COVID-19, a Hazard Group 3 (HG3) pathogen that can cause severe human disease. The United Kingdom’s Health Security Agency (UKHSA) classifies SARS-CoV-2 as a notifiable organism, and COVID-19 as a notifiable disease (2026).

‘FRSMs [Surgical Masks] have never been considered either adequate or suitable equipment for protection against inhalable or respirable risks under COSHH.’
‘In those school-rooms where ventilation is imperfect and the air impure, six sevenths of the money expended to educate a child is wasted.’ ❂ The Ventilation and Warming of School Buildings (1887) By Gilbert B. Morrison Published by D. Appleton and Company, New York. 1887. Accessed 10 Apr 2024 Preface (p.xxii) ❦ ‘I am fully convinced that people are prematurely dying by thousands simply from a lack of correct and positive convictions concerning impure air; for, when the true nature of a danger is fully appreciated, the requisite means to avert it will generally be found.’ ❂ Chapter II: The Effects Of Breathing Impure Air (pp.20-23) ❦ ‘Impure air is also believed by the best authorities to be one of the principal causes of epidemics. Dr. Carpenter, than whom there is no abler authority, says: “It is impossible for anyone who carefully examines the evidence to hesitate for a moment in the conclusion that the fatality of epidemics is almost invariably in precise proportion to the degree in which an impure atmosphere has been habitually respired.” The Board of Health of New York conclude that forty per cent of all deaths are caused by breathing impure air. In view of such alarming facts, this same board declares: “Viewing the causes of preventable diseases, and their fatal results, we unhesitatingly state that the first sanitary want in New York and Brooklyn is ventilation .” Direct experiment proves that the air in our school-rooms is impure in almost all cases, and in a majority of them to a degree far beyond the danger line. In view of these facts, and the results as proved by the authorities above cited, why is it regarded by the public with such indifference? When a school-house is blown down by a hurricane, killing and maiming a score of children, it is justly regarded as a great calamity; a vacation is given to quiet the excited fears of parents and children; investigating committees are appointed to locate the responsibility, and the faces of the whole populace are blanched with apprehension. Why is this? Why does the intelligent parent send his child to a school-room poorly ventilated and crowded with children, some of whom are breathing into a stagnant air the germs of disease and death, while others, from unwashed bodies, are delivering into it their deadly emanations, and all without a protest on the part of those even who provide proper hygienic conditions at home? It is because the effects of the one are immediate, occupy little time, the number killed can be actually counted, and the exact magnitude of the calamity estimated all at once. In the other case the process is slower, but of far greater extent; the actual results are by the general public less definitely known, and custom and attention to other matters divert the attention, and the deadly destruction of the innocents by impure air goes on silently, constantly, and powerfully. While noisy demonstrations like that of the cyclone attract attention, and inspire fear and terror, it is in the silent forces that the danger lies. Nature’s most destructive forces, as well as her strongest constructive ones, are silent in their operations; but when Science detects a silent, insidious enemy to human welfare, it is not only our duty to assume an attitude of self-defense and self-protection, but it should be regarded as folly not to do so.’ ❦ On high CO₂ levels connected to poor performance in schools: ‘The effects of breathing impure air thus far considered are pathological, but it has its pedagogical and economical aspects. Every observing teacher knows the immediate relation between the vitiated air in the school-room and the work he wishes the pupils to perform. Much of the disappointment of poor lessons and the tendency to disorder are due directly to this cause. The brain unsupplied with a proper amount of pure blood [oxygen] refuses to act, and the will is powerless to arouse the flagging energies; the general feeling of discomfort, dissatisfaction, and unrest which always accompanies a bad state of the blood. From an economical standpoint it would, of course, be impossible to estimate the financial waste of breathing impure air, but it can not but be enormous. In any discussion of the feasibility of incurring the additional expense of the most perfect ventilation, this loss occasioned by the want of such ventilation must not be ignored.’ ❂ Chapter III: The Air (pp.25-26) ❦ On ventilation, air filtration, and the super-spreading of diverse diseases in classrooms: ‘Wherever an unusual amount of unwholesome matter is being evolved, there especially should the purifying conditions be present; air in such places, to remain pure, must be changed in rapid succession, in order that dilution, diffusion, and oxidation may fulfill their legitimate functions. In a school-room the contaminating process can not but be rapid, and wherever ample provision is not made for rapidly changing the air of the room a dangerous condition of affairs is sure to exist. Bacteria of many forms, and spores of fungi, are also found in the air, and all these organisms are known to thrive in the organic impurities found in the air.’ ❂ Chapter IV: Examination Of The Air (p.33) ❦ On measuring CO₂ levels as a proxy to establishing content of (infectious) re-breathed air: ‘A complete analysis of impure air comprehends the quantitative and qualitative tests for carbonic [sic] dioxide, free ammonia, and other nitrogenous matter, oxidizable matters, nitrous and nitric acids, and hydrogen sulphide; but for ordinary practical purposes the determination of the CO₂ is by far the most important, and is ordinarily the only one which need be made. While the poisonous qualities of the air are not wholly due to the presence of the CO₂ per se, the amount of this gas found to be present is, in air made impure by respiration, generally a good measure for other impurities to which the poisonous quality is principally due. Owing to this fact, a careful test for the amount of CO₂ contained in a given atmosphere is generally the only one which need be made where air is tested merely to determine its respiratory purity.’ ❂ 📖 (Accessed 10 Apr 2024 ~ D. Appleton & Company / Google Books) The Ventilation and Warming of School Buildings ➤ ❂ My thanks to Maarten De Cock for alerting me to this gem of a book. ➲

‘The very first canon of nursing... the first essential to the patient... is this: to keep the air he breathes as pure as the external air, without chilling him .’ ❂ Notes on Nursing (1860 edition) By Florence Nightingale First Published 1859. Revised edition reprinted in 1860 by Harrison of Pall Mall Accessed 19 Feb 2024 ❦ Chapter I – Ventilation and Warming ‘The very first canon of nursing, the first and the last thing upon which a nurse’s attention must be fixed, the first essential to the patient, without which all the rest you can do for him is as nothing, with which I had almost said you may leave all the rest alone, is this: TO KEEP THE AIR HE BREATHES AS PURE AS THE EXTERNAL AIR, WITHOUT CHILLING HIM. Yet what is so little attended to? Even where it is thought of at all, the most extraordinary misconceptions reign about it. Even in admitting air into the patient’s room or ward, few people ever think where that air comes from. It may come from a corridor into which other wards are ventilated, from a hall, always unaired, always full of the fumes of gas, dinner, of various kinds of mustiness; from an underground kitchen, sink, wash-house, water-closet, or even, as I myself have had sorrowful experience, from open sewers loaded with filth; and with this the patient’s room or ward is aired, as it is called – poisoned, it should rather be said. Always air from the air without, and that, too, through those windows, through which the air comes freshest. From a closed court, especially if the wind do not blow that way, air may come as stagnant as any from a hall or corridor. I know an intelligent humane house surgeon who makes a practice of keeping the ward windows open. The physicians and surgeons invariably close them while going their rounds; and the house surgeon, very properly, as invariably opens them whenever the doctors have turned their backs. I have known a medical officer keep his ward windows hermetically closed, thus exposing the sick to all the dangers of an infected atmosphere, because he was afraid that, by admitting fresh air, the temperature of the ward would be too much lowered. This is a destructive fallacy. To attempt to keep a ward warm at the expense of making the sick repeatedly breathe their own hot, humid, putrescing atmosphere is a certain way to delay recovery or to destroy life.’ ❂ ‘I have known cases of hospital pyæmia quite as severe in handsome private houses as in any of the worst hospitals, and from the same cause, viz., foul air. Yet nobody learnt the lesson. Nobody learnt anything at all from it.’ ❂ ✪ C-19: On schools ‘Of all places, public or private schools, where a number of children or young persons sleep in the same dormitory * , require this test of freshness to be constantly applied.’ * [ C-19 Note: You might substitute ‘sleep’ and ‘dormitory’ with ‘study’ and ‘classroom’ in this section.] ‘If it be hazardous for two children to sleep together in an unventilated bedroom, it is more than doubly so to have four, and much more than trebly so to have six under the same circumstances. People rarely remember this; yet, if parents were as solicitous about the air of school bedrooms as they are about the food the children are to eat, and the kind of education they are to receive, at school, depend upon it due attention would be bestowed on this vitally important matter, and they would cease to have their children sent home either ill, or because scarlet fever or some other “current contagion” had broken out in the school. There are schools where attention is paid to these things, and where “children’s epidemics” are unknown.’ ❂ ✪ C-19: Offices, shops, factories, and other workplaces ‘How much sickness, death, and misery are produced by the present state of many factories, warehouses, workshops, and workrooms!’ ‘How much sickness, death, and misery are produced by the present state of many factories, warehouses, workshops, and workrooms! The places where poor dressmakers, tailors, letter-press printers, and other similar trades have to work for their living, are generally in a worse sanitary condition than any other portion of our worst towns. Many of these places of work were never constructed for such an object. They are badly adapted garrets, sitting-rooms, or bedrooms, generally of an inferior class of house. No attention is paid to cubic space or ventilation. The poor workers are crowded on the floor to a greater extent than occurs with any other kind of over-crowding. The constant breathing of foul air, saturated with moisture, and the action of such air upon the skin renders the inmates peculiarly susceptible of the impression of cold, which is an index indeed of the danger of pulmonary disease to which they are exposed. The result is, that they make bad worse, by over-heating the air and closing up every cranny through which ventilation could be obtained. In such places, and under such circumstances of constrained posture, want of exercise, hurried and insufficient meals, long exhausting labour and foul air – is it wonderful that a great majority of them die early of chest disease, generally of consumption? Intemperance is a common evil of these workshops. The men can only complete their work under the influence of stimulants, which help to undermine their health and destroy their morals, while hurrying them to premature graves. Employers rarely consider these things. Healthy workrooms are no part of the bond into which they enter with their work-people. They pay their money, which they reckon their part of the bargain. And for this wage the workman or workwoman has to give work, health, and life. Do men and women who employ fashionable tailors and milliners ever think of these things? And yet the master is no gainer. His goods are spoiled by foul air and gas fumes, his own health and that of his family suffers, and his work is not so well done as it would be, were his people in health. And the time will come when it will be found cheaper to supply shops, warehouses, and work-rooms with pure air than with foul air.’ ‘And the time will come when it will be found cheaper to supply shops, warehouses, and work-rooms with pure air than with foul air.’ ❂ ✪ C-19: On ‘air-tests’, and measuring CO₂ as a proxy for estimating prevalence of airborne disease indoors ‘Dr. Angus Smith’s air-test, if it could be made of simple application, would be invaluable to use in every sleeping and sick room. Just as without the use of a thermometer no nurse should ever put a patient into a bath, so, if this air-test were made in some equally simple form, should no nurse, or mother, or superintendent, be without it in any ward, nursery, or sleeping-room. But to be used, the air-test must be made as simple a little instrument as the thermometer, and both should be self-registering. ‘...the air-test must be made as simple a little instrument as the thermometer, and both should be self-registering.’ The senses of nurses and mothers become so dulled to foul air that they are perfectly unconscious of what an atmosphere they have let their children, patients, or charges sleep in. But if the tell-tale air-test were to exhibit in the morning, both to nurses and patient and to the superior officer going round, what the atmosphere has been during the night, I question if any greater security could be afforded against a recurrence of the misdemeanour.’ ❂ ✪ C-19: ... And back to the school-room, testing its air, and combatting airborne pathogens ‘And, oh! the crowded national school! where so many children’s epidemics have their origin; and the crowded, unventilated work-room, which sends so many consumptive men and women to the grave; what a tale its air-test would tell! We should have parents saying, and saying rightly, “I will not send my child to that school. I will not trust my son or my daughter in that tailor’s or milliner’s workshop, the air-test stands at ‘Horrid.’” ‘We should have parents saying, and saying rightly, “I will not send my child to that school... the air-test stands at Horrid .”’ And the dormitories of our great boarding schools! Scarlet fever would be no more ascribed to contagion but to its right cause, the air-test standing at “Foul.” We should hear no longer of “mysterious dispensations,” nor of “plague and pestilence” being “in God’s hands,” when, so far as we know, He has put them into our own. The little air-test would both betray the cause of these “mysterious pestilences,” and call upon us to remedy it.’ ❂ ❦ Chapter II – Health of Houses ‘There are five essential points in securing the health of houses:– Pure air. Pure water. Efficient drainage. Cleanliness. Light. Without these, no house can be healthy. And it will be unhealthy just in proportion as they are deficient. To have pure air, your house must be so constructed as that the outer atmosphere shall find its way with ease to every corner of it. ‘To have pure air, your house must be so constructed as that the outer atmosphere shall find its way with ease to every corner of it.’ House architects hardly ever consider this. The object in building a house is to obtain the largest interest for the money, not to save doctor’s bills to the tenants. But, if tenants should ever become so wise as to refuse to occupy unhealthily constructed houses, and if Insurance Companies should ever come to understand their interest so thoroughly as to pay a Sanitary Surveyor to look after the houses where their clients live, speculative architects would speedily be brought to their senses. As it is, they build what pays best. And there are always people foolish enough to take the houses they build. And if in the course of time the families die off, as is so often the case, nobody ever thinks of blaming any but Providence for the result. Ill-informed medical men aid in sustaining the delusion, by laying the blame on “current contagions”. Badly constructed houses do for the healthy what badly constructed hospitals do for the sick.’ ‘Badly constructed houses do for the healthy what badly constructed hospitals do for the sick.’ ❂ ❦ Conclusion ‘The whole of the preceding remarks apply even more to children and to puerperal women than to patients in general. They also apply to the nursing of surgical, quite as much as to that of medical cases. Indeed, if it be possible, cases of external injury require such care even more than sick. In surgical wards, one duty of every nurse certainly is prevention. Fever, or hospital gangrene, or pyæmia, or purulent discharge of some kind may else supervene. If she allows her ward to become filled with the peculiar close fœtid smell, so apt to be produced among surgical cases, especially where there is great suppuration and discharge, she may see a vigorous patient in the prime of life gradually sink and die where, according to all human probability, he ought to have recovered. The surgical nurse must be ever on the watch, ever on her guard, against want of cleanliness, foul air, want of light, and of warmth.’ ‘In surgical wards, one duty of every nurse certainly is prevention.’ ❂ 📖 (Accessed 19 Feb 2024 ~ Original text copied from FiftyWordsForSnow.com) Notes on Nursing (1860) ➤ 📖 (Accessed 19 Feb 2024 ~ Original scanned pages from Google Books) Notes on Nursing (1860) ➤ ❂
❦ LitCovid is the most comprehensive online resource on SARS-CoV-2 / COVID-19, providing access to 417,800+ relevant articles on PubMed. The library of scientific articles is updated daily, and categorised by different research topics (e.g. transmission), as well as geographic locations. ➲ Date accessed: 18 Feb 2024 . ❂ ❦ Useful Categories ✪ Transmission ➤ Characteristics and modes of SARS-CoV-2 transmission. ✪ Prevention ➤ Prevention, control, response and management strategies. ✪ Long Covid ➤ Post-COVID-19 Conditions/Complications (PCC) / Post-Acute Sequelae of COVID-19 (PASC). ✪ Case Reports ➤ Descriptions of specific patient cases. ✪ Treatments ➤ Treatment strategies, therapeutic procedures, and vaccine development. ✪ Forecasting ➤ Modelling, and estimating the trend of SARS-CoV-2 spread. ❂ ➲ LitCovid Online Library ➤ © 2024 National Institutes for Health (NIH) / National Center for Biotechnology Information (NCBI) / U.S. National Library of Medicine (NLM USA).

❦ Mitigation = ‘Lessening the force or intensity of something unpleasant; the act of making a condition or consequence less severe.’ 1. Clean indoor air . The priority should be air filters in schools and hospitals . New ventilation and air filtration standards for all public spaces . Grants made available to businesses to upgrade ventilation and air filtration . 2. FFP2/3 [N95/N99] respirators (masks) in all healthcare settings . 3. Free Covid vaccines available to everyone. 4. Wider access to Covid anti-viral treatments . 5. Free LFT/PCR testing . 6. Improved Covid surveillance , including wastewater monitoring and Long Covid prevalence . 7. Paid sick-leave , so that people don’t go to work when ill. 8. Respirators (masks) on public transport , including flights . 9. Better support and treatments for Long Covid patients . ... and last, but by no means least: 10. A public education campaign on the long-term risks of Covid – and why people should do more to protect themselves. ❦ Addendum : Allocate adequate research funding for a sterilising vaccine as well as treatments/cure for Long Covid . ❂ © 2024 Cat in the Hat . ➲
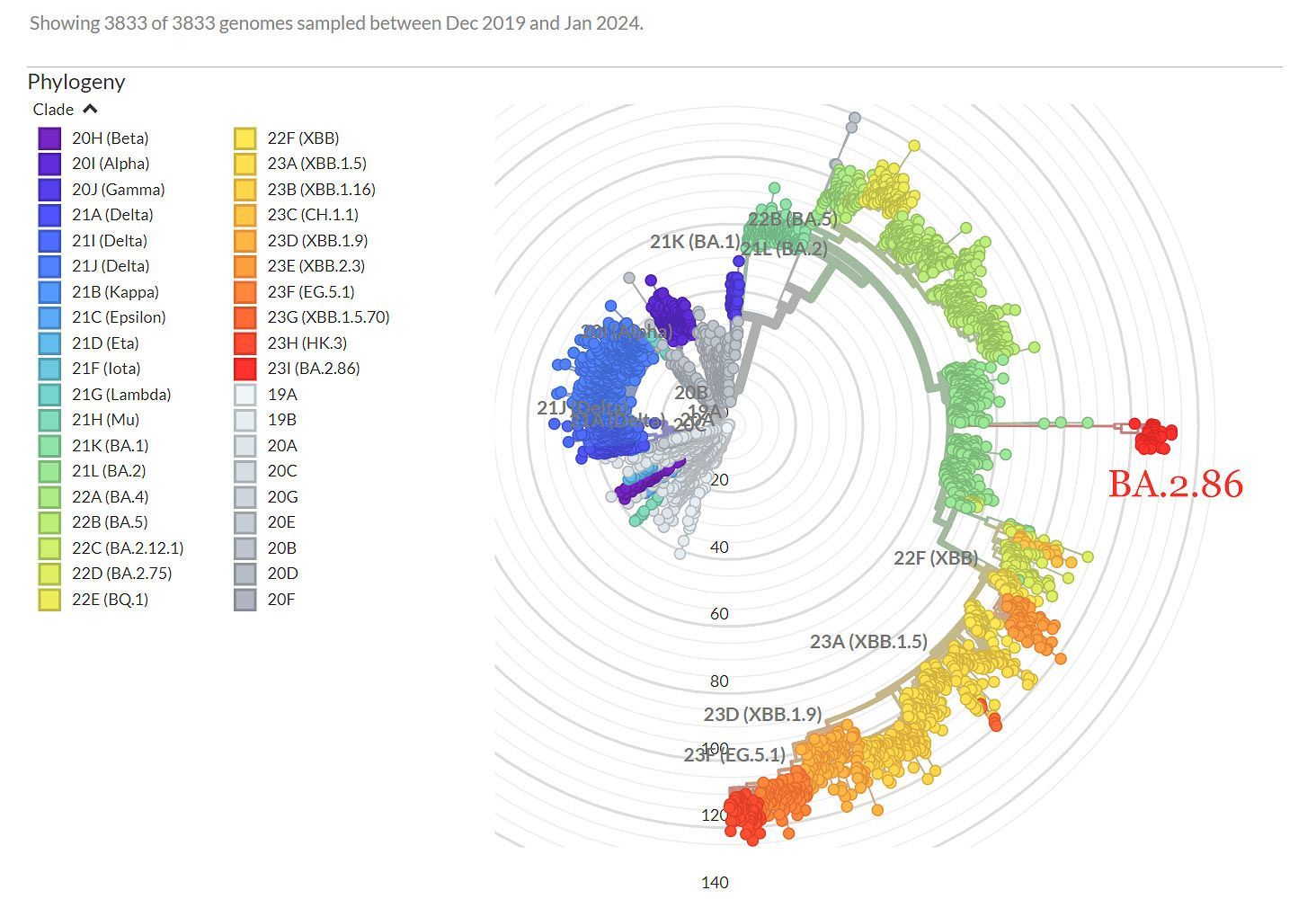
❦ Genomic epidemiology of SARS-CoV-2 with subsampling focused globally since pandemic start. All data and data visualisation by © 2025 NextStrain.org / GISAID.org .
❦ Mike Honey’s Variant Visualiser (COVID-19 Genomic Sequence Analysis). The region of ‘Oceania/Australia’ is set by default, as the visualiser was created by Mike Honey , a Data Visualisation and Data Integration specialist in Melbourne, Australia. ➲ Choose your country by clicking on the ‘ Continent, Country, Location ’ dropdown menu in the top-right-hand corner . The variant visualiser is free to use, and is automatically updated every time you open the link. ❂ © 2024 Mike Honey .

❦ “I met a nice lady – a ward patient – yesterday who, seeing my [ FFP3 ] respirator [ high-filtration ‘mask’ ] , promptly put on her surgical mask. So instead of diving straight in to asking what was most concerning her and how I could help, I opened up a bit about infection control in hospitals. I explained how, because of a lack of respirators, March 2020 saw NHS leaders downgrade PPE for all non-ICU staff. ❂ PPE : Personal Protective Equipment. I then reminded her of the amazing DHSC 2020 and 2021 campaigns on airborne transmission of SARS2 (the green-and-black smoke ones) – and I had to point out that every IPC Lead Nurse had since had to switch off their brain and forget what they knew – and while at work, to only protect ICU staff. ❂ DHSC : Department of Health and Social Care (UK). ❂ IPC : Infection Prevention and Control. I explained that the individuals responsible for the original IPC downgrade were now authors of the national manual on IPC (NIPCM), which sets the standard for infection control in hospitals, and this manual states that airborne transmission is ‘not a thing’ for SARS2 (AGP only). ❂ NIPCM : The UK’s National Infection Prevention and Control Manual. ❂ AGP : Aerosol-Generating Procedure, ie. intubation. So hospitals are destined to be unsafe spaces thanks to the NIPCM, and the surgical mask that she was wearing was OK (ish) to help protect me – but did very little to reduce her risk of SARS2 inhalation. However, she was in a single room (an extra, and not meant as a ward-bed space – but you know, >100% occupancy forever means that you need to use your imagination) – and she already had the window open. She was appalled at what healthcare workers were being put through. She was appalled at the on-going lies. She was appalled at the possible level of harm to patients and staff from such lies. She then went on to tell me how a weekend visitor of hers had just tested positive for Covid. She was worried that they had hugged and chatted, and that she might have got infected. She’s a switched on lady, too. Lives with a medic who has the windows open all the time (“It’s freezing at home”). So I explained about the CleanAirStars.com site. About HEPA filtration being a low energy and low-cost way to remove all airborne pathogens , and to make home a safer place for... • Covid • Flu • RSV • Norovirus • Fungi, etc. etc. The list goes on and on. — “Wow, that’s like magic!” We had a very nice chat. And then we talked about her heart. I just wish I could have this same conversation with each and every NHS CEO and IPC Lead Nurse. I’d ask some questions. I’d want to know why they aren’t protecting staff as they should. I’d want to know why they aren’t protecting patients as they should. I’d want them to know that they are in breach of UK legislation . And I’d want to look them in the eye and ask them to show compassion to the powerless: to staff, and patients. Help us please. Do whatever you can to counter the lies, and to help protect the NHS. Thank-you.” ✾ © 2024 Dr. David Tomlinson (NHS Consultant Cardiologist) ➤
❦ Q . Why is it important for me to know if I have a COVID-19 infection? ❦ A . If you don’t recover well, it can help your doctor to know if you’ve had a COVID-19 infection – so that they can more effectively treat any of your on-going symptoms. It also helps you to be conscious of the fact that contact with other people might hurt, permanently damage, or kill them.

‘It is accepted that COVID-19 can be and is spread by the airborne route. The recent evidence given at the UK COVID-19 Inquiry clearly shows that aerosol transmission is a significant, and almost certainly the dominant, route of transmission for COVID-19.’ The British Medical Association (22 Dec 2023)
‘The RCN is urging healthcare employers to assess the risk posed by COVID-19 and put appropriate safeguards in place for patients and staff. WHO [has] advised healthcare workers and health facilities to implement universal masking in health facilities, as well as appropriate masking, respirators and other personal protective equipment for health workers caring for suspected and confirmed COVID-19 patients; and to improve ventilation in health facilities.’ ✾ ❦ We’ve contacted chief nursing officers in all four UK countries and the UKHSA to find out what action will be taken in response to WHO’s statement on a new COVID-19 variant of interest. The RCN is asking for a revision to current guidelines , to introduce universal implementation of the two measures advised by the World Health Organization (WHO) to help protect healthcare staff against COVID-19. Earlier this week, in light of the new COVID JN.1 variant, WHO advised healthcare workers and health facilities to: implement universal masking in health facilities , as well as appropriate masking , respirators and other personal protective equipmen t for health workers caring for suspected and confirmed COVID-19 patients ; improve ventilation in health facilities . The existing national infection prevention and control manuals don’t require standardised masking for COVID-19, and decisions on respiratory protective equipment are left to local risk assessments. This is now inconsistent with WHO’s latest advice . We also have concerns about the adequacy of ventilation in general ward and outpatient areas within hospital buildings and believe that action must be taken to assess and improve this. Although evidence suggests that the global public health risks from the new variant are low, WHO has warned that onset of winter could increase the burden of respiratory infections in the Northern hemisphere. This comes when there are already unsustainable pressures on the health service. Figures show that there has been a rise in COVID-19 cases and hospitalisations , and the RCN argues that without proper protections , ill health could continue to rise in nursing staff and impact their ability to deliver safe and effective patient care . WHO has advised that it is continuously monitoring the evidence and will update the JN.1 risk evaluation as needed. The RCN is urging healthcare employers to assess the risk posed by COVID-19 and put appropriate safeguards in place for patients and staff . Our COVID-19 workplace risk assessment toolkit aims to help assess and manage the risks associated with respiratory infections such as COVID-19, highlights the duties of nursing staff in specific roles (such as health and safety reps), has advice for employers and leaders, and provides the latest information on risk assessment. ❂ 📖 (21 Dec 2023 ~ Royal College of Nursing / RCN Magazine) COVID JN.1 variant: RCN seeks assurance on new PPE advice ➤ © 2023 Royal College of Nursing (RCN).
❦ ‘Due to its rapidly increasing spread , WHO is classifying the variant JN.1 as a separate variant of interest ( VOI ) from the parent lineage BA.2.86 . It was previously classified as VOI as part of BA.2.86 sublineages. Based on the available evidence, the additional global public health risk posed by JN.1 is currently evaluated as low. Despite this, with the onset of winter in the Northern Hemisphere, JN.1 could increase the burden of respiratory infections in many countries. ➲ Read the risk evaluation: ‘Tracking SARS-CoV-2 variants’ . WHO is continuously monitoring the evidence and will update the JN.1 risk evaluation as needed. Current vaccines continue to protect against severe disease and death from JN.1 and other circulating variants of SARS-CoV-2, the virus that causes COVID-19. COVID-19 is not the only respiratory disease circulating. Influenza, RSV and common childhood pneumonia are on the rise. ➲ WHO advises people to take measures to prevent infections and severe disease using all available tools . These include: • Wear a mask when in crowded, enclosed, or poorly ventilated areas, and keep a safe distance from others, as feasible. • Improve ventilation . • Practise respiratory etiquette – covering coughs and sneezes. • Clean your hands regularly. • Stay up-to-date with vaccinations against COVID-19 and influenza, especially if you are at high risk for severe disease. • Stay home if you are sick . • Get tested if you have symptoms, or if you might have been exposed to someone with COVID-19 or influenza. ✻ ➲ For health workers and health facilities , WHO advises : • Universal masking in health facilities , as well as appropriate masking , respirators and other PPE for health workers caring for suspected and confirmed COVID-19 patients . • Improve ventilation in health facilities. Note : Updated 19 Dec 2023 with additional information for health workers and facilities. ’ ❂ 📖 (19 Jan 2023 ~ WHO / World Health Organization) World Health Organization (WHO) Media Advisory for the COVID-19 variant of interest (VOI) JN.1 ➤ © 2023 WHO / World Health Organization. ❦ Date accessed : 11 Jan 2024 .
❦ “Unless we reduce the transmission of Covid-19 through societal non-pharmaceutical interventions (such as cleaning indoor air) and/or the deployment and uptake of second-generation vaccines, attrition of healthcare will reach a tipping point. This tipping point – which may well happen within the next year – will lead to a global decrease in quality of available healthcare services, which in turn will lead to increased morbidity and mortality from all causes. Every government needs to reduce transmission. The denial of this problem will not change the outcome. Policymakers need to understand this.” ❂ © 2023 Conor Browne ➲

➲ I’ll be frank here. What’s the point of formatting this NHS document, and providing an easy-to-read, easy-to-access résumé for you, when every single healthcare worker that I’ve come across in the United Kingdom doesn’t actually believe: a. that SARS-CoV-2 is a highly dangerous, life-threatening, life-altering, biphasic, systemic, neurovascular pathogen; or b. that the laws of physics do, actually, happen to apply to aerosol-driven airborne pathogens – so why waste my time on providing you with (probably legally-binding) solutions? You can’t even recognise the problem yet. * ➲ File under ‘ Increasing Anosognosia & Executive Dysfunction ’. Read the bulletin yourself. Pick it apart. There’s a link below if you can be bothered. Blow it. Hang the whole show. Care for your patients (and yourselves and your own families), or don’t bother. I simply don’t care anymore. Je m’en fous, moi. M’en fiche. * [ As of 25 July 2025. ] ❦ Applicability ‘This NETB applies to all healthcare spaces with ventilation requirements .’ Objective ‘To provide additional technical guidance and standards on the use of UVC devices for air cleaning in healthcare spaces .’ Status ‘The document represents advice for consideration by all NHS bodies .’ ❂ 📖 (2 Oct 2023 ~ NHS England) NHS Estates Technical Bulletin (NETB 2023/01B): Application of ultraviolet (UVC) devices for air cleaning in occupied healthcare spaces: guidance and standards ➤ ✻ Accessed: 4 Dec 2023. ➲ Date Bulletin published: 9 May 2023. ➲ Date Bulletin last updated: 2 Oct 2023 . © 2023 NHS England.
❦ Chris Whitty, from the Covid Inquiry: “The one situation... that you would ever aim to achieve herd immunity is by vaccination . That is the only situation that is a rational policy response.” And yet... the UK is no longer offering vaccines to the vast majority of its working-age population. According to the JCVI member Dr Adam Finn, the UK’s strategy going forward is that: “... most under 65’s will now end up boosting their immunity not through vaccination, but through catching Covid many times .” ➲ (24 Sep 2023 ~ BBC) What you need to know about Covid as new variant rises ➤ Let me translate: The stated aim is to get infected over and over and over again... to protect against being infected over and over and over again! How does this make any sense at all? The government has decided that it is not good “value for money” to actually give the boosters out – even for the age groups who have already had Covid vaccine doses purchased for them (for example, the 50-65 year olds) – so millions of doses [8.5 million] are now destined to be binned, rather than being used. ➲ ‘COVID VACCINE: COST EFFECTIVENESS ASSESSMENT. For the first time ever, the UK government has used a ‘bespoke, non-standard cost-effectiveness assessment’ to decide who would be eligible for the Covid booster this Autumn. In this thread, I explore how this assessment was undertaken…’ ➤ Meanwhile, in many other countries, the booster is open to anyone who wants it . No strict eligibility criteria. Just step forward and get protected. Let’s take a look at a few: 1. THE USA : Covid booster available to EVERYONE aged 6 months and older. The CDC (USA’s Centers for Disease Control ) recommends that everyone ages 6 months and upwards get the updated COVID-19 booster to protect against serious illness. The new vaccine targets the most common circulating variants, and should be available later this week. The full details are here ➤ . 2. CANADA : Covid booster available to EVERYONE aged 6 months and older. Full details are here ➤ . 3. FRANCE : Covid booster available to EVERYONE. Full details are here ➤ . 4. BELGIUM : Covid booster available to EVERYONE. Full details are here ➤ . 5. JAPAN : Covid booster available to EVERYONE aged 6 months and older. Full details are here ➤ . Why is the UK falling so far out of step with so many other countries on their Covid vaccine strategy? How can they justify binning millions of purchased vaccine doses when there are many people who would gladly take them? ➲ ‘So what’s going to happen to the millions of purchased doses which now won’t be used? Well, here’s the real kicker... it seems they’re destined for the bin. A number of alternative uses have been considered, but the conclusion is: “THESE DOSES HAVE NO FEASIBLE ALTERNATIVE USE”. ’ ➤ If the UK government won’t fund deployment of the Covid jab to EVERYONE (as so many other countries do), then why isn’t there at least an option to buy it privately? This model already exists with the flu jab – why is there not the same option for Covid? © 2023 Cat in the Hat ➲
❦ “I accept that school boards ultimately do not care about the safety of their students and staff. But a HEPA air purifier costs less than a few days of sub coverage. Add a $1 mask/day x 180 school days, and that’s another day of sub coverage. You don’t incur the disruption to education delivery that happens when a sub comes in. You’re not potentially permanently disabling education workers. The “school boards are cash-strapped” excuse makes no sense when the solution to constant sickness is: “We’ve got more subs!”” © 2023 Amanda Hu . ➲
❦ Two million people living in this country have Long Covid, and there have been over 230,000 deaths due to Covid. That’s why masks are now commonplace, and people want to help protect each other ❤️. It’s why hospitals across the NHS are striving to do all they can to limit the spread of nosocomial Covid, recognising the increased risk of death it carries, wanting to limit Long Covid, as well as protect their staff in work ❤️. It’s why your workplaces and schools have introduced safer ventilation and clear policies to reduce outbreaks, to clearly communicate what’s happening, and protect generations of the future from a multi-system, vascular-driven illness ❤️. It’s why, instead of ignoring Covid, society has gathered together as one to help limit the devastating damage we have all witnessed, and why it has collectively said “no” to any further preventable death or disability from this pandemic by all taking simple, effective mitigations ❤️. © 2023 NHS Medical Consultant . ➲
❦ “It’s not like I’ve never seen people die of causes that are a result of their lifestyle... but it’s awful seeing people die as a result of other people’s lifestyles... and now that includes their healthcare provider! It feels very similar to watching people die from another person’s drunk-driving... That’s the closest similar situation I can think of. We are drunk-driving in healthcare... with a pathogen that has a 10% fatality rate in that setting.”
❦ “Dear economy enthusiasts... The only humane way to avoid locking down for airborne disease control ever again is to set up safer indoor-air infrastructure... globally. Everyone that is slowing down this process is asking for another lockdown. Or mass murder. More likely another lockdown though because in the end, if bird flu takes off or MERS has an interesting offspring... the public will not stomach as much death as the anti-lockdown and dirty-air proponents would like.”
❦ “Whenever I hear someone ask if we’re expected to continue masking in healthcare settings forever, I immediately think of Semmelweis – the man who discovered that healthcare workers’ dirty hands were causing fever and death in patients. The result of his discovery wasn’t the widespread implementation of hand hygiene though... Instead he was shunned, ostracized, lost his job and eventually institutionalized. It took around fifty years before the life-saving value of hand-washing was fully recognized in healthcare. Fifty years. It turns out that doctors didn’t take kindly to the idea that their own hands were unhygienic – and the source of disease and death for some of their patients. Despite the evidence, the denial was rampant and it was strong. The majority consensus was that Semmelweis was a crank... The resistance to the idea that the air we exhale while caring for patients can be unhygienic, and a source of illness and death for some, feels exactly the same to me. Despite the evidence, the denial is strong. Many prefer to cling to the status quo they knew before the pandemic. But that status quo was when we didn’t know better, and when we didn’t have such a virulent and dangerous new airborne pathogen in permanent circulation. Now that we do, and now that we know better, we should be willing to do better. So if the air we breathe can be unhygienic, and cause illness and death in our patients, and we know there’s a simple, effective solution – filtering it through a respirator – then it seems logical that this would become the new standard in our clinics, hospitals and long-term care facilities. Permanently. But as with Semmelweis’ experience, I expect that suggestion to get a lot of pushback, and for it to take a very long time for the medical field to accept that the old status quo is gone, and that masking in healthcare is the new normal. I just hope it won’t take another fifty years.”
❦ “Since the pandemic began, I have constantly made the argument that a healthy workforce is a necessity for a healthy economy. This, to me, is the definition of obvious. The same argument applies to education. I’m writing this because I’ve received a large number of messages and e-mails this week from parents who are being placed under extreme pressure by schools in an attempt to stop their children trying to avoid infection. Let me be very, very clear: education is extraordinarily important. Health is extraordinarily important. A child’s education will suffer if that child is unwell. Again, the definition of obvious. Parents should not be put in a position in which they are being forced to choose between their child’s health and their child’s education. It is a false dichotomy that mirrors the pernicious culture of presenteeism that is sadly still present in many workplaces. It’s also driven by the nature of box-ticking bureaucracies that always seek to maintain the status quo. This is both an ethical and pragmatic argument. Ethical, because placing pressure on parents to have to choose between access to education and near-certain infection of their children is morally wrong. And, believe me, I make moral statements carefully. Pragmatic, because if schools simply introduced air-filtration as standard, and encouraged parents to keep children with acute Covid off school, there would be far, far less transmission in schools – thus improving the quality of education for all. Again, the definition of obvious. Much like the economy, we need to employ medium- and long-term thinking now, rather than short-term thinking that clings to the status quo purely for its own sake. And remember, reduction of transmission in schools reduces transmission in the wider community. As such, this means that less adults are sick at any given time, which is also good for the economy. This is so clear that it baffles me that most policy-makers seem to fail to understand it.” © 2023 Conor Browne . ➲
❦ “There is no such thing as “personal risk assessment” for the vast majority of people. A tiny number of dominant personalities in your life (and it could be you) have decided what to do, and the rest will follow. Even those that are making the decisions are not making a personal risk assessment. They are making a group risk assessment and taking their whole family/community with them. People may not even realise this – that they have made the decision on behalf of their entire household/class/company... but they have... If there is no responsible public health leadership, someone else is leading... because that is how we work, by and large, as a species. Someone is in charge... someone is always in charge, and unfortunately... misinformation is rife.”
❦ “Yesterday someone confronted me about my social media content – saying that while I’m not wrong, I’m too radical. They asked me: — “OK. What happens once everyone agrees (that Covid reinfections are problematic ) – then what?” Then we clean the air. HEPA filters are not radical. I don’t know what they expected as an answer. We regulate water safety and food safety in an effort to decrease population rates of waterborne and foodborne illnesses. Having clean air standards to lower the rates of respiratory illnesses isn’t radical. It’s also not radical to suggest we keep masking in healthcare and in essential indoor spaces so that the disabled, the high-risk, the elderly and their families can safely enjoy community life again. Wearing a respirator is not hard. Wearing 4-inch heels is hard, and I do that all the time for no good reason other than vanity. Accessibility is not radical. Advocating in favor of a public health response to an on-going threat is not extremism. SARS-CoV-2 is the Number One infectious-disease killer in Canada, and our excess deaths are still high. It’s not radical to think we should do something about it... It’s also not radical to advocate for the bare minimum in terms of public health education campaigns on Long Covid / Post-Covid Syndrome, and airborne transmission. Empowering people through education is not radical. It’s just wild for me that someone would think my Covid public health advocacy is radical when, in reality, they agree that we should clean the air, mask in healthcare and other essential places, and educate the public. Did they think I was going to answer with “lockdowns” ? Or is the radical part that I care enough to advocate out loud? Even when it’s not popular? Even when there’s an increasingly intense push to frame Covid health advocates as radicals and extremists? Or maybe I’m a radical because I don’t value brunch or maskless grocery shopping enough to risk Long Covid, or to betray my values? Is it radical that my physical health and my integrity are important enough to me that I’m at peace with my decision not to conform to societal expectations? If you’ve misclassified people you actually don’t disagree with as “radicals” in your mind, you should take half a second to examine how and why that happened, and re-examine your assumptions. There’s nothing radical about clean air and compassion. We don’t lack scientific consensus. The pandemic is complicated because we lack values consensus .”
❦ “What if Covid has been causing mass cognitive impairment and we are all living in an increasingly stupid society? Mad things could happen with that: imagine if hospitals got rid of masks or people started to believe Covid was just a cold? I know that’s far-fetched, but imagine!” ❂ © 2023 NHS Palliative Medicine Consultant .
❦ ‘The magnitude of the outbreak illustrates how younger children infected from diverse pediatric facilities can be a major source of widespread household transmission with the potential to facilitate community transmission in the era of the Omicron variant. With highly transmissible variants such as the Omicron (B.1.1.529) variant of concern (VOC) and its subvariants becoming dominant globally, the role of children in transmission dynamics needs to be elucidated to take tailored public health and social measures for the control of outbreaks and pandemics. On epidemiological investigation, frequent and intimate interactions among children, along with inadequate indoor ventilation, were commonly observed in pediatric facilities. Given the practical challenges of behavior modification among pediatric populations, including consistent and correct mask use and physical distancing, the environmental control interventions, such as improved ventilation systems, upper-room ultraviolet germicidal irradiation, or portable high-efficiency particulate air-filtration appliances, may offer sustained benefits in stemming the virus transmission in pediatric facilities.’ ❂ 📖 (20 Apr 2023 ~ Yonsei Medical Journal) Widespread Household Transmission of SARS-CoV-2 B.1.1.529 (Omicron) Variant from Children, South Korea, 2022 ➤ © 2023 Park et al / Yonsei Medical Journal.
❦ ‘ Aerosol spread of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is a major problem in hospitals , leading to an increase in supplementary high-efficiency particulate air ( HEPA ) filtration aimed at reducing nosocomial transmission.’ ➲ Note : A nosocomial infection – also referred to as a healthcare-associated infection ( HAI ) – is an infection acquired during the process of receiving healthcare that was not present during the time of admission. ‘Air-cleaning units ( ACUs ) reduce microbial contamination in ward air , demonstrating that the application of a combined HEPA/UV-C ( ultraviolet-C ) ACU on an older adult inpatient ward reduced airborne particulate matter (PM) levels substantially , most notably in the size range associated with respiratory viruses, such as SARS-CoV-2. Therefore, such devices may be applicable not only to pathogens traditionally considered airborne , such as measles and tuberculosis , but also where aerial dissemination contributes to the transmission of fungal and bacterial infections , such as with Clostridioides difficile spores. This study found that airborne particulates associated with human activity migrated considerable distances around the ward , indicating that social-distancing measures alone are unlikely to prevent the transmission of respiratory viral infections and possibly other infections that are aerially disseminated. Collectively, this suggests that appropriately-sized ACUs have the potential to reduce nosocomial infections , especially in inadequately ventilated hospital wards.’ ❂ 📖 (23 Feb 2023 ~ Journal of Hospital Infection) Impact of supplementary air filtration on aerosols and particulate matter in a UK hospital ward: a case study ➤ © 2023 Journal of Hospital Infection .
❦ ‘A recent US Centers for Disease Control and Prevention (CDC) analysis of 1.4 million children aged under 12 years and 1.7 million adolescents aged 12-17 years found increased rates of asthma, myocarditis and cardiomyopathy, cardiac dysrhythmias, diabetes, renal failure, venous thromboembolism, and coagulation disorders in children with laboratory-confirmed COVID-19 compared with children without COVID-19. These increased risks (excluding asthma) were also experienced by adolescents with COVID-19, who were additionally at increased risk of pulmonary embolism. Although uncommon or rare, such outcomes suggest children are not spared the cardiovascular and metabolic sequelae of COVID-19. Reinfection is common and SARS-CoV-2 spreads readily in schools in the absence of mitigation measures, such as the use of masks, portable HEPA air cleaners, and improved ventilation. Notably, better ventilation has wider benefits, including improved academic performance. (A poorly-ventilated classroom can be equivalent to a student skipping breakfast.) The COVID-19 pandemic is not over. On-going commitment to a public health strategy informed by the precautionary principle is required. This will deliver wide-ranging social, economic and health benefits.’ ❂ 📖 (20 Feb 2023 ~ The Medical Journal of Australia) Balancing the medical and social needs of children during the COVID‐19 pandemic ➤ 📖 Related: (April 2021 ~ The Lancet COVID-19 Commission) The Lancet COVID‐19 Commission Task Force on Safe Work, Safe School, and Safe Travel. Designing infectious disease resilience into school buildings through improvements to ventilation and air cleaning ➤ © 2023 Zoë Hyde / The Medical Journal of Australia.
❦ “The way I see it, if somehow all the data on the cumulative risk of death, hospitalisation, disability, heart attacks, strokes, etc. with repeat Covid infections turns out to be wrong, I will have worn a mask for longer than I needed to and missed a few social events. I’m OK with that. Whereas if I decided to follow the crowd instead of the available science, and the available data turns out to be right about the risks of cumulative Covid infections, then I’d be facing high odds of poor health, disability, and premature death. Those are very high stakes. When the stakes are high, you can’t afford to be wrong. So seeing ‘experts’ wave around the absence of certainty as their justification for choosing the high-stakes position, when the high-stakes position is the one that requires the most certainty… it’s just so absurd. On the other hand, I can pull up multiple scientific studies on how Covid (and the loss of parents/primary/secondary caregivers) harms children…”
📖 A rapid review of Supplementary air filtration systems in health service settings. September 2022.
❦ ‘The aerosol spread of SARS-CoV-2 has been a major challenge for healthcare facilities and there has been increased use of supplementary air filtration to mitigate SARS-CoV-2 transmission. Appropriately-sized supplementary room air filtration systems could greatly reduce aerosol levels throughout ward spaces . Portable air filtration systems, such as those combining high efficiency particulate air (HEPA) filters and ultraviolet (UVC) light sterilisation, may be a scalable solution for removing respiratory viruses such as SARS-CoV-2. This rapid review aimed to assess the effectiveness of supplementary air cleaning devices in health service settings such as hospitals and dental clinics (including, but not limited to HEPA filtration, UVC light and mobile UVC light devices) to reduce the transmission of SARS-CoV-2. One systematic review (Daga et al. 2021), three observational studies (Conway Morris et al. 2022, Thuresson et al. 2022, Sloof et al. 2022), one modelling study, (Buchan et al. 2020) and two experimental studies (Barnewall & Bischoff 2021, Snelling et al. 2022) were found. Outcome measures included symptom scores, presence of SARS-CoV-2 RNA in sample counts, general particulate matter counts, viral counts, and relative risk of SARS-CoV-2 exposure. From real world settings, the systematic review assessed the effectiveness of HEPA filtration in dental clinics (Daga et al. 2021), two additional observational studies assessed HEPA and UV light in UK hospital settings (Conway Morris et al. 2022, Sloof et al. 2022) and one observational study included mobile HEPA-filtration units in Swedish hospitals (Thuresson et al. 2022). Studies were published from 2020 onwards. Real-world evidence suggests supplementary air systems have the potential to reduce SARS-CoV-2 in the air and subsequently reduce transmission or infection rates but further research, with study designs having lower risk of bias, is required. HEPA filters alongside UVC light could provide the most notable reductions in SARS-CoV-2 counts , although the supporting evidence relates to HEPA/UVC filtration, and this review does not provide evidence on the effectiveness of other potential supplementary air filtration systems that could be used. Evidence is limited on the optimum air changes per hour needed and the positioning of air filtration units in rooms.’ Acronyms : ➲ HEPA High efficiency particulate air * * High efficiency particulate air = A designation used to describe filters that are able to trap 99.97% of particles that are 0.3 microns or larger . ➲ UVC Ultraviolet C ➲ CFD Computational Fluid Dynamics ➲ ACH Air-change per hour ❂ 📖 (26 Oct 2022 ~ Health & Care Research Wales / Welsh Government / MedRxiv / Pre-print) A rapid review of Supplementary air filtration systems in health service settings. September 2022 ➤ © 2022 Health & Care Research Wales / Welsh Government.
❦ “Engineers raised the entire city of Chicago in the 1850s so they could install a sewage system in response to repeated epidemics of typhoid and cholera, but please tell me again how you don’t believe engineers can retrofit buildings with proper ventilation and filtration in 2022.”
❦ A new type of ultraviolet light can efficiently kill airborne microbes , such as those which cause COVID-19 , a study has found after successful trials. The result suggests that this light, known as Far-UVC , could be used to significantly reduce the risk of person-to-person indoor transmission of hospital-acquired infections as well as airborne diseases such as COVID-19 and influenza . Published in Nature Scientific Reports, the research carried out by the Universities of Leeds, St Andrews, Dundee and Columbia University in New York with NHS Tayside is the first study to measure the performance of Far-UVC under full-scale conditions. The researchers released an aerosolised bacteria known to be harder to inactivate than the SARS-CoV-2 virus which causes COVID-19, into a room-sized chamber and then tested the level of microbial reduction when it was exposed to the Far-UVC light. Reduced levels The trials, held at a bioaerosol facility at the University of Leeds, found that Far-UVC light rapidly and continuously reduced levels of airborne microbes with a 92% – 98% reduction recorded even when the bacteria aerosol was continuously introduced. Dr Louise Fletcher, of Leeds’ School of Civil Engineering, said: “Our bioaerosol facility at Leeds provides a unique environment for this type of research. “The facility is a sealed chamber the size of a single-occupancy hospital room where different types of building ventilation and devices can be implemented to test the potential effectiveness of approaches like Far-UVC in a full-scale situation.” The study was led by the University of St Andrews. Dr Kenneth Wood, from the School of Physics and Astronomy. He said: “Our trials produced spectacular results, far exceeding what is possible with ventilation alone or using conventional filter-based air cleaners. “In terms of preventing airborne transmission, Far-UVC lights could make indoor places as safe as being outside on the golf course at St Andrews.” Killing all COVID-19 variants Dr David Brenner, of the University of Columbia in New York, said: “We now know that Far-UVC light is superbly efficient at killing airborne microbes . And based on our earlier studies we have very strong evidence that is will be equally good at killing all the COVID-19 variants, past, present and future, as well as the “old fashioned viruses” like influenza and measles . “So, by simply adding UV light to the conventional lighting in indoor rooms, we can quickly kill all the airborne viruses in the room and so protect ourselves against person-to-person indoor disease transmission.” The team received a grant of £136,000 from the UK Health Security Agency to carry out the trials - and they will continue their research into the safety and efficacy of Far-UVC lights through two recently awarded grants totalling £270,000 from the UK Health Security Agency and NHS Scotland Assure . ❂ 📖 (23 Mar 2022 ~ University of Leeds) Anti-viral light neutralises COVID-19 ➤ © 2022 University of Leeds.
❦ “I plan to continue to wear a mask in all public indoor spaces, not just because I care about others, but because I care about my own health too. Both my short- and long-term health. So I don’t want to catch Covid. I certainly don’t want to catch it multiple times. No thank-you. The “We’re all going to catch it eventually” mindset doesn’t really make sense to me as a reason to throw in the towel since even if I catch it, immunity isn’t durable – and there’s no evidence that we’re only risking long Covid, clotting issues, lung damage, etc. the first time. Not only do we roll the dice with each infection, but what if the damage from repeated infections is cumulative? I haven’t seen any evidence that multiple Covid infections is a safe long-term plan. Did I miss that study? Or am I in it? Because in that case I choose the control group. And for many of us, our sense of self-preservation and desire to protect people we care about is very strong. So if the government wants to see me out and about maskless like it’s 2019, then make it safe for me to do that. Contain the virus. Otherwise, I’ll to continue to choose my health and the health of my family over most other things until science comes through for us. I can wait.”
Ryan Hisner pulls apart the real-life Animal Farm theatre playing out between Man, Pig and The Economy in his 2022 essay on swine, clean air, and bringing home the bacon. ✾ ❦ “What should be a higher priority for society: preventing pigs from becoming sick, or preventing human illness? Personally, I place a higher value on preventing human illness. I think most would agree. Why, then, are pig barns far better ventilated than schools? An airborne virus has killed 900,000 Americans, and has left countless others suffering from Long Covid along with its chronic, and perhaps permanent, mental and physical afflictions. We know that ventilation and the filtration of indoor air prevents illness. The manifold benefits of improved ventilation are well-documented and uncontroversial. Professor Don Milton has been publishing studies for over twenty years showing that improved ventilation reduces respiratory illnesses and absences, though his findings were largely ignored. Yet we’ve done almost nothing to improve air filtration and ventilation in schools, workplaces, restaurants, and other buildings. The USA’s CDC (Centers for Disease Control and Prevention) gives lip service to ventilation – but has issued no minimum ventilation requirements, and offers no specific guidance. 📖 (26 Feb 2021 ~ CNN Health) CDC must encourage better ventilation to stop coronavirus spread in schools, experts say ➤ On the other hand, great cost and effort is put into ventilating and filtering the air in pig barns in order to prevent disease outbreaks. Let’s compare the ventilation and air-filtration of pig barns with buildings inhabited by human beings. First, note that airborne spread of Porcine Reproductive and Respiratory Syndrome (PRRS) was readily accepted based on circumstantial evidence and lab studies. French farms even installed HEPA filtration systems in pig barns, despite “no hard data to support” their use. Contrast this with the stubborn, year-long denial of airborne Covid spread by the WHO and CDC, despite abundant evidence. The precautionary principle is obeyed when pigs’ health is at stake, but not when human health is at risk. Incredibly, droplet dogma still reigns supreme in some places. Many are still fighting against appallingly ignorant public officials and nonsensical guidelines in Australia. [Insert ubiquitous poster from your hospital, doctor’s surgery, pharmacy, bowling alley or supermarket extolling the virtues of hand-washing and hand-sanitiser in a pandemic essentially driven by aerosol transmission .] Some officials haven’t gotten the memo yet: Covid is airborne . Many careful, controlled studies of ventilation and air-filtration in livestock facilities have been carried out, and the cumulative evidence compiled leaves little doubt of their effectiveness at preventing disease in farm animals. One of many examples: 📖 (July 2006 ~ Canadian Journal of Veterinary Research) Further evaluation of alternative air-filtration systems for reducing the transmission of Porcine reproductive and respiratory syndrome virus by aerosol ➤ In contrast, before Covid, research on ventilation, air-filtration and disease in human dwellings was pretty sparse. Linsey Marr, Don Milton, Julian Tang, Yuguo Li and others were lone voices in the wilderness, shouting into a void, and ignored by the CDC and the WHO. For buildings that humans inhabit, enforced minimum ventilation requirements are almost non-existent. The HVAC* in a school or nursing home can be completely non-functional, creating a superspreader environment, and with no legal consequences. * HVAC = Heating, Ventilation, and Air Conditioning. This is not hypothetical. Here is one documented instance in which all 226 residents in a Canadian nursing home contracted Covid, resulting in over 70 deaths. 📖 (14 May 2020 ~ CBC News) Investigators look into catastrophic outbreak that infected all residents of TMR seniors' home, killing 70 ➤ The cause? A non-functioning ventilation system. And this was a less transmissible, pre-Alpha SARS-CoV-2 variant. 📖 (15 May 2020 ~ Radio Canada) Un CHSLD infecté à 100%, avec un système de ventilation en panne, préoccupe Québec ➤ The same private company owned another nursing home in which 96% of residents and 116 employees caught Covid, leading to the death of 66 residents. I think we can surmise that the ventilation in this facility was also very poor. Why were the ventilation systems in these nursing homes not audited? Because such auditing is simply not done – not in nursing homes, schools, workplaces or restaurants. Ventilation and air-filtration recommendations exist, but not enforced standards. They’re essentially voluntary. What about pig barns? While there are no legal requirements, the ventilation and air-filtration systems at these facilities are assiduously checked every day by a worker whose sole duty is to inspect and maintain the ventilation equipment. 📖 (12 Nov 2016 ~ National Hog Farmer) Hog barn filtration system audits imperative to disease control ➤ No aspect of the system is left unchecked. “Look for any gaps or openings that would allow dirty air in... Make sure chutes collapse properly, creating a good seal.” “Cracked fan housings or a broken shroud” are checked for, and “weep holes plugged with a rubber stopper...” But daily inspection is only the start. In addition, at least once a month, a system filtration technician (SFT) audits the ventilation system, coaching the on-site manager. Another monthly audit is performed by the herd veterinarian, who guides the SFT. In contrast, human dwellings (such as nursing homes) are virtually never audited, even during a pandemic. It apparently requires a court order for such an audit to occur. Are HVAC systems in human-occupied buildings well maintained? HVAC expert Jeffrey Siegel: “The best HVAC in the world performs poorly when it’s not well maintained, and the usual standard is ‘not well maintained’.” The same article* describes an HVAC unit installed upside-down in a large store, making it impossible to change the filter, meaning that “... the air inside the store would be that much crummier”. It was like “a thousand other HVAC mistakes” Siegel has seen: “... dampers supposed to admit outside air into a building rusted open or shut, badly-installed filters letting air pass around their edges, forced-air fans running 18% of the time. In theory, HVAC heats and air-conditions. In practice, it doesn’t always ventilate... or filter.” * 📖 (9 Nov 2020 ~ Wired) The Next Covid Dilemma: How to Make Buildings Breathe Better ➤ What sort of air filters are used for pig barns? First, a mesh net catches larger objects in the air, such as feathers. Then the air goes through a MERV 8 ‘pre-filter’. This pre-filter is of a higher grade than the filters used in many schools, which are MERV 7. After passing through the MERV 8 pre-filter, air entering pig barns is filtered by MERV 15 air filters – similar to the filters used in hospitals. Very few schools, workplaces, nursing homes or restaurants use anything above MERV 11. MERV 15 is unheard of. Does such high-quality ventilation and filtration of pig barns reduce disease outbreaks? Of course it does, as the extensive literature on livestock-facility ventilation and air-filtration attests. 📖 (May 2012 ~ Viruses) Evaluation of the long-term effect of air filtration on the occurrence of new PRRSV infections in large breeding herds in swine-dense regions ➤ However, there is a potential problem: what if some of the dirty air from the human-occupied office building on a farm were to leak into the pig barn? Perish the thought! To allow pigs to breathe the same filthy air breathed by humans would be unthinkable. Therefore, pig farms are designed so that none of the filthy air from the farm’s human office is allowed to contaminate the pristine, highly-filtered air of the pig barn. (“If there is dirty air in the office, it will stay in the office.”) The notion of providing pig-quality air to the office is considered so absurd that it doesn’t merit consideration. After all, if the health of the workers on a farm is improved, this doesn’t affect profits. A sick pig, on the other hand, hurts the bottom line. Priorities... One article on the ventilation and air-filtration of pig barns notes a peculiar “side benefit” of improving the pigs’ air: human workers notice the better air, and seem healthier for it. How much healthier? No-one knows, as such trivial topics as worker health are not researched. So why is the air quality in human buildings so poor? Why haven’t greater efforts been made to improve indoor air quality (IAQ), the enormous benefits of which are well-known and uncontroversial? After all, we regulate water and food safety. Why not indoor air? The WHO recommends schools and other buildings have at least 6 air changes per hour (ACH). A typical school HVAC provides less than 1 ACH. IAQ experts recommend CO2 levels be less than 800 ppm (or less than 700 ppm in a pandemic), but CO2 levels regularly reach much higher levels in schools. I’ve occasionally registered levels near 3000 ppm; others report readings higher than 4000 ppm. What about hotels? I stayed in a room at the Disney Caribbean Resort Hotel with my brother. CO2 reached well over 3000 ppm each night. I did a CO2 decay study, and found that the room got 0.11 air changes per hour. Not good. It’s long past time to greatly improve ventilation and air filtration by imposing serious, enforced IAQ standards in nursing homes, schools, workplaces and other public spaces. Many aerosol and IAQ experts have been calling for this for a long time. 📖 (14 May 2021 ~ Science) A paradigm shift to combat indoor respiratory infection ➤ Only recently have their calls gained traction. The vast majority of people would be much better off if IAQ were improved through better ventilation and filtration. We spend the majority of our lives indoors. Proper air filtration and ventilation would enormously improve the air we breathe. When we think of air pollution, we usually think of lung damage. But polluted air damages all organs of the body. With cleaner air, brain function would improve; heart attacks and strokes would fall; illness would be reduced. It works for pigs. It can work for humans, too. Air pollution is possibly the single largest health problem in the world. It causes the loss of more years of life than alcohol and narcotics, unsafe water, HIV, malaria, and war combined. Cleaning the air we breathe is essential. However, the pecuniary interests of the 1% of landlords, real-estate magnates, business owners, and capitalists in general might not be so well-served. Installing better ventilation systems and air filters in human dwellings might put a dent in their investment returns – an unthinkable notion. To sum up. Improving indoor air quality in human dwellings merely improves the health and well-being of humans – a minor consideration – while improving air quality in pig barns improves profits: a sacred objective, and the chief aim of life under capitalism.” ❂ Related : 📖 (10 Aug 2020 ~ The Conversation) How to use ventilation and air filtration to prevent the spread of coronavirus indoors ➤ Related : 📖 (28 Sep 2020 ~ Quartz) What everyone should know about ventilation and preventing Covid-19 ➤ ❂ © 2022 Ryan Hisner . ➲
❦ I keep saying that someday I’ll write a book about the struggle to bring an engineering perspective to infection prevention and control in healthcare. For now... just an essay. Is there anything worse than knowing that there are oceans full of icebergs ahead; how easy it is to engineer systems to detect and steer around them; but not being able to get the owners of the liners (or anyone in command) to listen as you blindly head straight for them? I’ve been advocating for engineering solutions and standards for air, water and surfaces in healthcare facilities to lower disease transmission for over 30 years. The irony of being accused by out-of-touch ID/PH/IPAC/Epi * of epistemic trespassing before and during the pandemic is gobsmacking. * ID = Infectious Diseases / PH = Public Health / IPAC = Infection Prevention and Control / Epi = Epidemiology. I started with single patient rooms. In pre-pandemic Canada, we had the highest HAI* rate in OECD * – one in ten inpatients – and the lowest beds and lowest single rooms per capita. * HAI = Hospital-Acquired Infection, also known as a nosocomial infection, is an infection that patients get in healthcare facilities while receiving treatment for other medical or surgical conditions. * OECD = Organisation for Economic Co-operation and Development. We also had sicker patients. Studies now show that single-patient rooms cut infection rates in half. Ten years ago, Canada began moving to primarily single-patient rooms for new hospital builds – although not a hundred percent as hospitals won’t give up preferential private-room billing to insurance companies. In 2007, we formed a small group of volunteers to create a Canadian National Standard for Plume Evacuation – source control to prevent airborne transmission of disease in ORs * . * OR = Operating Room. Despite nurses’ complaints, we couldn’t get support – until doctors started getting genital warts in their noses. We helped ISO * develop a similar global standard which was published in 2014. * ISO = International Organization for Standardization. Because laser and electrocautery smoke is clearly visible, and there are now national and international standards, the practice of source control in ORs is now well-accepted. Unlike smoke, our breath is not visible – and there are no national or international standards yet for pathogen-free air. However, the principle of air extraction would work in ICUs * and patient rooms just as well as ORs. * ICU = Intensive Care Unit. Copper was registered as an antimicrobial in 2008, 50 years after silver. Over the past ten years, countless studies have shown efficacy, persistence, durability and the safety of copper surfaces – but the ID community pushes back with objective conclusions like “... Too good to be true”. While ID/IPAC has no budget of their own to implement engineering measures in hospitals, in Canada they can (and most often do) scuttle initiatives in Engineering and Facilities Management, and in Environmental Services departments, to introduce new technologies and materials to combat HAIs. In 2011, I pursued the concept of combining continuous and high-frequency bioburden reduction of surfaces to prevent fomite transmission. Copper could provide ‘continuous’ reduction on high-touch surfaces, while UV * (if automated) could provide ‘high-frequency’ reduction on all surfaces. * UV = Ultraviolet (UV) radiation. In 2014 we launched AutoUV – built-in fixtures that detected occupancy, monitored whether doors were open or closed, and dosed rooms every four hours and after every exit. As expected, it works. It can’t not work. And after seven years in the field, it’s been shown to be extremely safe. Bathrooms can be the source of half of disease spread in hospitals. C diff * can be colonized in air after every toilet flush. Aerosols drift for minutes to hours. Intestinal and respiratory diseases are often spread through toilet aerosolization. * C. diff , also known as Clostridioides difficile or C. difficile , is a gram-positive bacterium that can cause diarrhoea and colitis. AutoUV? Bathroom source-control. Today, there are thousands of units in use across Canada – and the Ontario Ministry of Health has made AutoUV a standard-of-care for new hospital builds. MOHLTC * now mandates and funds AutoUV. * MOHLTC = Ontario Ministry of Health and Long Term Care. Hooray. But IPAC stubbornly pushes back against the use of AutoUV. In other ironic news, Health Canada is cutting off use of open-air UV in healthcare, including Upper Air UV – in the middle of an airborne pandemic – due to a flood of household UV devices that are being sold retail and online that don’t work, don’t have safety certificates, or produce [dangerous] ozone. In 2014 I co-founded CHAIR – the Coalition for Healthcare-Acquired Infection Reduction – a group of scientists, engineers, ID doctors and industry partners working together to engineer air, water and surfaces in order to lower HAIs. We naively thought that we could achieve an 80 percent decrease in preventable, environmental HAIs with new technologies and materials. We knew legacy industry players in chemical disinfection would be a challenge. We had no idea that the biggest battle would come from the ID/IPAC community itself. I watched in horror at the denial of airborne transmission of 2003 SARS at a plenary session in Toronto in May 2014. Playing to the crowd in a purposeful, dismissive and comedic way, the speaker claimed that “SARS is not airborne . The droplets fall to the floor within six feet.” Dr Yu, of Hong Kong Public Health, had only just re-analyzed and re-published the Amoy Gardens study six months earlier on the 10-year anniversary reaffirming airborne transmission of [the original 2002-2004] SARS. When I challenged the speaker, he exclaimed: — “Oh, don’t worry. I know him. He's changed his mind.” In 2014, an ID doc from PHO * presented at a Toronto IPAC Education Day. * PHO = Public Health Ontario. He claimed that Ebola was definitely not airborne . When challenged with a study showing transmission between caged and separated laboratory primates, he replied: — “Well, monkeys have long arms. Besides, they can spit.” In a follow-up from me: “There’s airborne transmission of PRRV * in hogs between factory farms kilometers away, and documented in Veterinary journals...” * PRRV = Porcine reproductive and respiratory syndrome virus. — “I don’t read those journals.” — “Would you like me to send you some articles?” — “Don’t bother.” They don’t want to know. Hospitals are a global network of MDRO * incubators. * MDRO = A multidrug-resistant organism (MDRO) is a germ that is resistant to multiple types of antibiotics, making it difficult to treat and cure infections. CDI * and MRSA * initially tend to spread in hospitals before seeding community-acquired versions. Sinks and drains are known sources of contamination, especially via the aerosol route. Pathogens are getting more virulent – including MDRO/CPE/CRE/CPOs and C auris. * CDI = Clostridioides difficile infection (CDI or C-diff), also known as Clostridium difficile infection, is a symptomatic infection due to the spore-forming bacterium Clostridioides difficile. * MRSA = Methicillin-resistant Staphylococcus aureus (MRSA) infection is caused by a type of staph bacteria that's become resistant to many of the antibiotics used to treat ordinary staph infections. Water contamination and aerosolization, and bacterial, fungal and biofilm reservoir control = Engineering. Progressive examples: ➲ In Calgary Health Region: UV all incoming water? No Legionella. Self-disinfecting sinks? Electrocatalytically-split H2O into OH-, O-, O3 and H2OH = Disinfectant. ➲ In Ontario, the Ministry of Health now funds and mandates self-disinfecting sink and drain technologies. However, IPAC/ID continue to push back against new technologies. So why write this essay? Because the current struggle to recognize airborne transmission, and the engineered solutions, is part of an epic struggle. We’ve seen how much resistance there has been in almost two years. The entrenchment started a century ago, as most of us know. But the struggle has been about much more than “airborne” . It’s a struggle for epistemic control; for critical thinking; for evaluation to first principles; the applied use of deductive reasoning; politics; economics; tension between careerism, and the Precautionary Principle. Many in ID/PH have fought against engineering measures, but now are giving up on fighting the virus at all. It’s important to not give into the temptation of accepting that “We just have to live with it,” or that “It’s endemic now” – or “It's mild” . No . Not acceptable. COVID-19 is airborne. It’s very manageable. Wear an N95 [FFP2 respirator] in occupied spaces until case counts are near zero. Make indoor air safe – ventilate, filter it, and use UV. Set national and international standards for safe indoor air. Set a goal of elimination – first regional, then national, and then global. ❂ © 2021 Barry Hunt . ➲
❦ ‘There is robust evidence supporting the airborne transmission of many respiratory viruses , including measles virus, influenza virus, respiratory syncytial virus ( RSV ), human rhinovirus ( hRV ), adenovirus , enterovirus , severe acute respiratory syndrome coronavirus ( SARS [-CoV-1] ), Middle East respiratory syndrome coronavirus ( MERS-CoV ), and SARS-CoV-2 . A growing body of research on COVID-19 provides abundant evidence for the predominance of airborne transmission of SARS-CoV-2 . This route dominates under certain environmental conditions, particularly indoor environments that are poorly ventilated , an observation that implicates solely aerosols because only aerosols – and not large droplets or surfaces – are affected by ventilation. Additional precautionary measures must be implemented for mitigating aerosol transmission at both short and long ranges , with a major focus on ventilation , airflows , air filtration , UV disinfection , and mask fit . Transmission of SARS-CoV-2 has occurred in healthcare settings despite medical [blue surgical/FRSM] masks (designed for droplets not aerosols) and eye protection, which illustrates the need for proper personal protective equipment ( PPE ) and layering multiple interventions against airborne transmission, especially in high-risk indoor settings . Implementing effective ventilation systems reduces airborne transmission of infectious virus-laden aerosols. Strategies such as ensuring sufficient ventilation rates and avoiding recirculation are advised. Carbon dioxide sensors can be used as indicators of the build-up of exhaled air and serve as a simple way to monitor and optimize ventilation . Aerosol sensors can also be used to assess HEPA and HVAC aerosol filtration efficiencies, which are key to lowering infections caused by virus-laden aerosols. Assuring a minimum ventilation rate of 4 to 6 air changes per hour ( ACH ) and maintaining carbon dioxide levels below 700 to 800 ppm have been advised, although the ventilation type and airflow direction and pattern should also be taken into account. Increasing the efficiency of air filtration in HVAC systems , stand-alone HEPA purifiers , or implementing upper room UV disinfection systems can further reduce the concentrations of virus-laden aerosols. These interventions are critical strategies for helping end the current pandemic and preventing future outbreaks. The risk of outdoor transmission may rise with increased lifetime and transmissibility of viruses, such as certain variants of SARS-CoV-2. Aerosolization of virus-containing wastewater and hospital fecal discharges also poses potential outdoor exposure risks , which should not be underestimated.’ ❂ 📖 (27 Aug 2021 ~ Science) Airborne transmission of respiratory viruses ➤ © 2021 Science .
❦ from ‘The Lancet COVID-19 Commission Task Force on Safe Work, Safe School, and Safe Travel’ : ‘Buildings play a critical role in minimizing, or conversely exacerbating, the spread of airborne infectious diseases.’ ‘Buildings play a critical role in minimizing, or conversely exacerbating, the spread of airborne infectious diseases. COVID-19 outbreaks occur indoors, and within-room long-range transmission beyond two meters (six feet) has been well documented in conditions with no masking and low ventilation rates. However, the relationship between building systems and airborne infectious disease transmission predates SARS-CoV-2, the virus that causes COVID-19. Building-related interventions have been shown to reduce the spread of many other airborne infectious diseases, including severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS), tuberculosis, measles, and influenza. Following the 2009 H1N1 influenza A pandemic, an epidemiological investigation at a boarding school in Guangzhou, China found that opening windows for outdoor air ventilation was the only control measure that had significantly protected against infection. Other research confirmed that enhanced outdoor air ventilation can reduce influenza and tuberculosis transmission in school buildings. Similarly, upper-room ultraviolet (UV) germicidal irradiation installed in Philadelphia-area schools substantially reduced measles spread during an epidemic. As of early 2021, no in situ research has evaluated the independent impact of ventilation and air cleaning for reducing the risk of COVID-19 transmission in schools. However, there are a number of studies in which enhanced ventilation was used as part of layered risk reduction strategy, resulting in the successful reduction of COVID-19 infections. For example, COVID-19 cases and mitigation strategies were tracked in schools in two cities in Missouri in December 2020. Schools that used a combination of mitigation strategies including improved outdoor air ventilation were found to have lower rates of transmission compared to the rest of the community. COVID-19 transmission among children in Baden-Württemberg, Germany was also rare in schools and childcare settings that employed mitigation strategies which included improved ventilation. Conversely, inadequate outdoor air ventilation has been explicitly implicated in several large COVID-19 outbreaks across various indoor environments. Case studies have included a choir rehearsal with poor ventilation and no masks; a meat processing facility with low air exchange rates and high rates of unfiltered recirculated air; a spin class without masks and inadequate air circulation; a bus with an air conditioning system on recirculating mode, and a restaurant with poor ventilation and an air conditioner that recirculated air through the dining room. These counterexamples demonstrate that building-level strategies, including ventilation and air cleaning, are key components of risk reduction strategies for airborne infectious diseases, including COVID-19. Schools are chronically under-ventilated.’ ✾ ‘Schools are chronically under-ventilated.’ ✾ 📖 (April 2021 ~ The Lancet COVID-19 Commission) The Lancet COVID‐19 Commission Task Force on Safe Work, Safe School, and Safe Travel. Designing infectious disease resilience into school buildings through improvements to ventilation and air cleaning. © 2021 The Lancet COVID-19 Commission .
❦ ‘First do no harm, “ primum non nocere ”, is a doctrine as old as medicine itself, frequently but probably inaccurately attributed to Hippocrates, the wise old man of our profession. Prevention of injury and illness is another significant aspect of medical practice. The profound impacts it has had on society, largely taken for granted in the industrialised world but less so elsewhere, are extraordinary; immunisation , sanitation , screening programmes , road safety initiatives – the list goes on – have changed our lives to degrees unimaginable even 30, let alone 100 years ago. Although it is an important component of our profession, it is underplayed in both training and our day‐to‐day activity . It is encouraging to know that it will be part of our new curriculum, despite the time constraints and rationalisation imposed by the modernising medical careers platform...’ ❂ 📖 (23 Apr 2007 ~ Geoffrey Hughes / Emergency Medicine Journal) First do no harm; then try to prevent it ➤ © 2007 Geoffrey Hughes / Emergency Medicine Journal.